Hearing minutes now posted: http://www.fda.gov/downloads/
On day 2 of the FDA Public Hearing, Impact of Approved Drug Labeling on Chronic Opioid Therapy, we heard much of the same from patient advocate PROPagandists. Perhaps the most bothersome to me at today’s hearing is that the FDA Panel allowed PROP advocate Avi Israel to speak on behalf of not one, not two, but three patient families with his personal added explicatives; it was a bit much after listening to the same thing yesterday. Certainly we all feel bad for families that have lost loves ones to opioid addiction, or suicide as was the case with his son, but this behavior needs to be separated from the issues at hand. He held up two tablets to the audience and said “I have synthetic heroin in this hand and ibuprofen in this hand. Which one would you take?” He was attempting to liken oxycodone to heroin, but of course was mistaken as I pointed out later (see below). He told the story of a 27 year old navy veteran who committed suicide and he blamed it on addiction to opioids; but he also disclosed that this victim had an ongoing history of hallucinations, paranoia, and suicidality. Hello…this sounds like untreated PTSD, a significant risk factor when prescribing opioids. If that is the case, once again, the issue at hand is education for prescribers and closer monitoring of the patient, not to make changes to the FDA indications for opioids.
On the upside, we heard from Dennis Capolongo representing the Arachnoiditis Society for Awareness and Prevention”. He pointed out the problems this patient population needs to endure and that a significant percent of epidural injections have poor outcomes for these patients. He also showed a very interesting correlate between increased opioid RX’s and increased arachnoiditis suggesting that many epidural failures resulting in arachnoiditis end up on chrionic opioid therapy. Perhaps this is in fact the case, but perhaps not. He did ask however that if label changes are made, that the FDA consider adding acceptable prescribing for chronic intractable non-cancer pain.
William Schmidt, an Industry Consultant and Kevin Nicholson from the National Association of Chain Drug Stores spoke in favor of not changing the labeling but taking other important measures; all the while, Dr. Kolodny was Tweeting about both of them. Dr. Schmidt actually showed pretty compelling evidence from a most reliable source, Dr. Gavril Pasternak, on the 20 mu-receptor variants associated with OPRM1 and COMT that cause patient variability in response to opioids.
We heard from Anita Roach, representing the Interstitial Cystitis Association and Rebecca Kirch of the American Cancer Society, both of whom advocated for chronic pain patients and allowable opioids and education. Fred Brason spoke on Project Lazarus, North Carolina and their efforts to reign in opioid misuse and educate providers…it sounds like regulatory agencies countrywide can learn from their success and experience. His presentation was quite compelling.
After the scheduled presentations, an Open Public Hearing ensued. At this point, I spoke and tried to dispel certain myths or half-truths presented over the past 2 days. Below is a pretty close recount of my comments.
Dr. Fudin’s FDA Hearing Comments: YOU MAY ACCESS THE VIDEO BY CLICKING HERE!
My name is Dr. Jeffrey Fudin. I am a Clinical Pharmacy Specialist at the Stratton VA Medical Center in Albany NY where I work in a comprehensive Pain Clinic and am Director of a PGY2 Pharmacy Pain Residency. I am an Adjunct Associate Professor of Pharmacy Practice at the Albany College of Pharmacy & Health Sciences, and Founder of PROMPT, a multidisciplinary group of healthcare providers which stands for Professionals for Rational Opioid Monitoring and PharmacoTherapy.
What I’m about to say is not the opinion of the Dept. of Veterans Affairs or the Albany College of Pharmacy & Health Sciences or Union University, but is consistent with much of PROMPTs opinion. In summary though, it is my opinion alone.
I have no disclosures to make in regard to this meeting, and I have financed my travel to this meeting myself.
In the spirit of good faith and maintaining an equal playing field, I’d like to point out that several presenters stated or displayed that they had no conflict of interest “with any pharmaceutical companies”. Considering some of the data we saw yesterday regarding Worker’s Comp, and considering some special interest groups OTHER than the pharmaceutical industry, I respectfully request that all participants presenting at this hearing be required for the record to disclose any and all funding sources for travel and related professional activities directly connected with this hearing and future hearings whether it be pharmaceutical industry related or otherwise, including but not limited to those organizations that could potentially have a financial interest in the reduction of prescriptions written for opioid therapy.
We have heard that oxycodone and heroin are practically one in the same chemically. While I don’t dispute this, I offer for the record that buprenorphine, while very safe in comparison to most opioids, is equally chemically similar to heroin. Furthermore, dextromethorphan is the methylated dextrorotatory analog of levorphanol, both of which are phenanthrene derivatives. To suggest that oxycodone or any other pure opioid is more or less similar without divulging all of the facts is misleading and does not serve any productive outcome other than riling the media and the families of patients that have already suffered and continue to suffer.
MORPHINE MAXIMUM DAILY DOSE
We heard yesterday that those patients receiving 100mg or more of morphine equivalents per day had a higher rate of death. But, that data is short-sighted considering that if this dose is prescribed, it is likely prescribed to a population of sicker patients compared to those on lower doses. All this data tells us is that there’s a higher correlation between persons receiving at least 100mg of morphine equivalents daily and death, compared to lower doses, BUT it does not tell us what that correlation is.
With specific regard to morphine equivalents, I want to share two recent projects…
The first was a publication this past December in the Journal of Pain and Palliative Care Pharmacotherapy entitled Rifampin reduces oral morphine absorption; A case of selection based on morphine pharmacokinetics. For purposes on this blog page, see this link for an explanation of that article.
A similar publication is underway with telaprevir that can have the opposite effect of INCREASING serum morphine and also affect methadone on the absorption side from the gut, through the BBB, and on the metabolic side as well.
These drug interactions directly affect the serum morphine levels without even considering patient variables from polymorphism. One could argue that based on drug interactions alone, serum morphine equivalent could be 75% higher or lower. [Explanation to panel…]
Recently I assigned a group of fifth year pharmacy students to convert five medications to morphine equivalent doses (See paindr.com blog, The Answer is Morphine 100mg Equivalent – Morphine Jeopardy for specific outcome data) using three different reference sources to include their choice of online conversion calculators, package inserts, textbooks, primary literature. There were 16 unique references used by 15 students. The dosing range from one source to another was huge.
The problem as presented at this hearing of substance abuse, misuse and addiction VERSUS the problem of pain management needs to be delineated. The commonality here is that education is essential, not only to prescribers for managing pain [Dr. Argoff’s presentation was discusses regarding appropriate therapies and inappropriate therapies for various pain types], but to recipients of these medications at the point of the prescriber. Equally important is that pharmacists cannot evade their responsibility of counseling upon the dispensing of a prescription by asking a patient to simply sign a statement saying that they refused counseling. An expansion of the REMS ETASU for transmucosal fentanyl products to the community pharmacy setting for all opioids could be a step in the right direction. But it can’t stop there…it should include the prescribers and a minimal knowledge base on how to interpret urine drug screens. It’s not enough to order these screens if the clinician does not have a clear understanding of their utility, the pitfalls and/or when serum analysis is useful.
Dentists should not be allowed to give refills on any C-III medication and they should be limited to a 48 hours supply for routine root canals and extractions. If there are more complex procedures, they should be required to enter a code to so designate that, as NSAIDs, if a medically acceptable option, are generally more effective. If that is not the case, they should so designate that in a code as well.
PERSPECTIVE
We’ve heard a lot of numbers and statistics, but let’s be honest with ourselves; More deaths are caused each year by tobacco use than by all deaths from human immunodeficiency virus (HIV), illegal drug use, alcohol use, motor vehicle injuries, suicides, and murders combined. I don’t see anyone limit the number of cigarettes that one can purchase or the nicotine intake from any consumers! But, this is on the table for opioids. (Centers for Disease Control and Prevention. Smoking-Attributable Mortality, Years of Potential Life Lost, and Productivity Losses—United States, 2000–2004. Morbidity and Mortality Weekly Report 2008;57(45):1226–8. AND McGinnis J, Foege WH. Actual Causes of Death in the United States. Journal of American Medical Association 1993;270:2207–12.
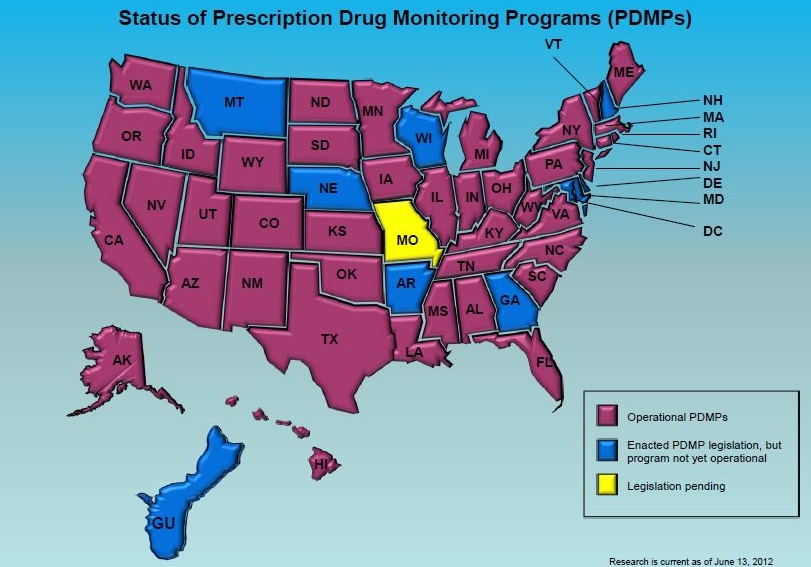
In closing, I wish to stress the importance of a prescription monitoring program that stretches across all states and allows prescribers and pharmacists to access real time data that must be evaluated prior to ordering or dispensing any controlled substance prescription, regardless of scheduling. Such an effort MUST include all federal government facilities including the DoD and the Veterans Administration, as opioids often find their way from federal institutions to the hands of civilians.
Limiting opioids by tying the hands of providers is not in the best interest of patient care and will likely cause a “whack-a-mole” effect resulting in an escalation of heroin use and/or other agents. The key is to work together and use computerization to better monitor where these drugs are coming from, where and when they are dispensed in real time. We must educate providers, pharmacists, and families on the risks and benefits of opioid therapy and expand the opioid REMs program.
I am a practitioner and pain sufferer. I would hope that the “experts” leave treating the patients to the relationship between the doctor and patient. I’ve had back surgery twice,and post-operatively, was taking 80mg oxycodone 4-5x/day. Not being opioid naive, I had no problems and am now down to oxycodone 20mg tid. A good relationship between a trained practitioner and the patient is more important than some expert who has a theory to tell everyone that all patients are created equal. When will they realize that patients aren’t like changing spark plus on the bmw. they’re all different. Smoking and alcohol contributes to more death than opioid ever will. Maybe they should limit how many beers you can buy in one day? (they’ll never do that, they won’t get re-elected if they mess with the alcohol or tobacco industry.)
This government is about maintaining control over the physicians and patients. I smell socialism in the air.
p.s. I too suffer from chronic pain and without medical help I also could not get out of bed. I crawled from the car to the house after doc appts. Forgot to say that….you know my condition but others here may not so sorry for not saying.
Don’t think I don’t care because I don’t post much but family emergencies have been overboard since my dad passed in November. I still read but am struggling right now…do appreciate your representation to keep things fair for those in cp
I haven’t had a chance to watch the videos, but I was wondering if any of the letters were read that people submitted to the forum? As a disabled chronic pain patient I couldn’t be there of course, but I was hoping some of the letters were read or at least looked at. One of my main points is, in America 15,000 people die from drug addiction (and for some reason this includes people who shoot themselves, which is I don’t think counts) compared to 100 million people in the US suffering from chronic pain. That alone should be enough to stop all this nonsense. I didn’t ask for this life, but my pain medications help improve my quality of life. It doesn’t take the pain away completely, but without it I would be in bed all day, useless, at 31 years old. No matter what, people are going to abuse drugs, or medications, or whatever gets them high, it’s been happening for thousands of years. Putting more regulations on everything will eventually lead to banning medications that help thousands and thousands of people.
Thank you for your support and understanding, it means a lot to us that are suffering daily.
The letters were reviewed by panel members on a separate forum.
Dr.Fudin,
I just finished watching all of the videos from the FDA meeting. I was wondering, have you watched the video of your speech? It is interesting and kind of funny because Avi Israel is giving you a dirty stare for the entire speech and Pete Jackson is repeatedly making comments to Ada Giudice behind you and making all sorts of angry/irritated gestures. Just made me laugh how the truth was able to get under their skin. It was refreshing to watch.
Interesting Andy! Can you provide the link here for everyone to see?
Here is the link:
http://www.tvworldwide.com/events/fda/130207/default.cfm
Under the section title “webcast archives,” scroll all the way down to the bottom and click on the video labeled “open public hearing,closing remarks.”
Dr. Fudin,
Do you think the FDA was receptive to the points made by you and other supporters of chronic pain patients? I am fairly upset at how under represented pain patients were. I do believe it is unfair that healthy people like Avi Israel were able to go and speak multiple times for multiple people. I also believe it is unfair that Canadian citizens like Ada Giudice-Tompson and Irfan Dhalla were allowed to speak. It is almost like PROP hijacked the hearing and turned it into a kangaroo court. Many chronic pain patients can’t travel to hearings like this testify because of their medical conditions or because they are poor. Chronic pain is not cheap to treat. I just really wish more pain patients were able to go to put a human face on the terrible diseases and accidents that leave people in chronic pain that requires opioids to treat.It would be devastating if the FDA accepted any of PROP’s proposals, especially since their arguments were all emotion and nothing substantial. I really hope the FDA does not make any decisions until they hear more input from chronic pain patients and not from an audience comprised mostly of anti-pain medicine extremists.
I guess the only thing I can do at this point is hope and pray that PROP fails. Anyways, thank you Dr.Fudin for attending the hearing and for your unwavering support of chronic pain patients.
Andy,
The FDA panel is comprised of pretty smart people. I suspect they saw through much of the rhetoric and will approach this fairly.
I wish there were a way someone could speak up and say that they were representing however many of us signed onto a statement written in advance. By definition, most of us who stand to lose the most in this struggle couldn’t possibly appear in person to speak up. THANK YOU for presenting such well-documented arguments and coherent rationale for what stands to affect so many of us.
It feels beyond ironic that anyone over 21 y.o. can access an unlimited amount of alcohol at any time, but physician-prescribed medication is where additional oversight is sought. Not to mention that we are witnessing, recently, how U.S. citizens of all political parties maintain that the option to bear some form of arms is our birthright, despite very well-known statistics re. accidental deaths in homes that contain handguns alone. And again, it is the relationship between specialist physicians and horribly pained patients that is deemed insufficient…
With extreme gratitude,
-D. Zucker
NSAIDs don’t work for me; I vomit and even had to be rushed to the ER after hours of intractable vomiting. NSAIDs provide ZERO pain relief. Opioids do work and they are the only thing that does. We need to keep opioids available for chronic non-cancer pain. Thank you, Dr. Fudin, for a balanced perspective.
Same here. I have severe neuropathy and opioids are the only treatment that work. They cut my pain down from an excruciating and unbearable eight to a slightly distracting three. When you’re in horrific pain, you take whatever relief you can get. I tried all the anticonvulsants and they either didn’t work or had terrible unmanageable side effects. I tried all the antidepressants as well and they did nothing. NSAID’s don’t work at all either. I know I am not alone. Why should I have to suffer in severe pain because my body is most receptive to opioid analgesics? Why should I have to suffer because some idiot abused drugs and passed away? The PROP proposals are basically attacking the true victims. Chronic pain patients like me are the true victims, not the drug abusers who knowingly abuse pain medicines. I don’t believe for one second the commonly used excuse ” (insert name here) did not know how dangerous these medicines were.” There are warnings plastered all over the medicine containers and there are thousands of ads across the United States warning about the dangers of abusing pain medicines. Not to mention that the dangers of pain medicine abuse are taught in most high schools.
The people who pass away from drug abuse have nobody to blame but themselves. Unfortunately, some bad decisions can be fatal. That is a fact of life. PROP is comprised of many doctors and health professionals who should be somewhat intelligent, yet somehow they can’t comprehend simple concepts like personal responsibility and free will.
Thank you Dr. Fudin for giving a balanced presentation of the opioid controversy. I appreciate your dedication to this issue.
This problem cannot be solved by changing the labeling, and needs a global comprehensive approach including education, coordination of services, and careful monitoring. Societal incentives to minimize inappropriate opioid usage needs to be implemented. Unfortunately, if the situation is “remedied” by regulatory statutes, it will lead to the undertreatment of pain by all medical providers, and the balloon will be pushed in another direction (ie illicit substance use, overutilization of emergency rooms or additional tests/ procedures/ surgery) which will further compound the problem.
Dr. Hoffberg:
Thank you for your insightful comments and dedication to pain patients and rehabilitation medicine as well.
Great Job yesterday at the meetings..Thank you for mentioning Dennis Capalongo’s presentation in your blog. I think Dennis did a great job addressing the needs of us, patients of arach. This disease is not well known and I hope to see the FDA start investigating this disease. Along with the many Meningitis Patients who are now being diagnosed with Arachnoiditis. This is beginning to be an epidemic and something needs to be done. I was diagnosed with Arach after I had a series of 3 Epidural injections in my lumbar spine to help treat the pain I was having with my recent DDD diagnosis. If only I knew then what I know now, I would have never got these injections. It has ruined my life, career, family and friends.
Most people could not even live with this disease. Herb Neeland and I both say it takes a strong person to deal with this disease! Thank You again for protecting us that suffer..
Becky
Thank you ror all the work you have done to finally get Arachnoiditis put in the spotlight even though briefly. I pray the FDA will start looking into the causes of our disease. There is no cure and the injections into our spines only cause more harm yet no one is trying to stop these practices. Please do not let scarred or angry greiving citizens take away our only means of getting some relief. We treasure every pill & would never sell or give even one away. This is not the way to stop prescription drugs from getting out on the streets.
Dr. Charles Burton, an expert who studied arach for many years & published “The Burton Report” stated that the pain of arachnoiditis is like that of spinal cancer but without the release of death (paraphrased).I agree with him.
Dr.Fudin,
Thank you very much for attending the FDA hearings and and being a voice of reason. I hope that they seriously consider what you had to say before making a decision which, if is in keeping with the requests of PROP, will have devastatingly negative impacts for those in this country living with chronic pain only responsive to opiates. One thing I don’t think any of the opposition has addressed is how to treat patients with chronic acute and severe pain who have bleeding disorders which rule out NSAIDs and any other strong anti-platelet drugs. I am certainly not the only patient in this category.
Thank you for all of your support for the pain patients in our country.
Lori
I want to thank you for going to bat for chronic pain patients like me. Unfortunately I have tried all other treatments to no avail. The only thing left for me are opioids, and I’m on too low of of a dose at that. I’m not asking to be pain free, I just want less pain. If the government gets involved, there rate of suicide will skyrocket. I truly hope they listen to reason.
Thank you again,
Jeanne Bierach
Call them out Jeff!
As a neuropsychiatrist who practices pain management, I wish I could have been there to provide “reinforcement”.
It sounds like the Straw Men were out in force. Lets keep highlighting the ill informed biases and prejudices of those who are imPROPer…
Thank you Dr. Fudin for your remarks today. I tried to get in to watch the live feed, but kept getting an error. I was told by tech support there was too many people watching the live feed. Hopefully, the FDA will make decisions based on sound judgement and science and not on emotions.
Dr. Fudin,
Thank you for your continued advocacy, time, and effort! I also want to thank you for this blog, and for giving people in pain a voice.
Nancy
Ridiculous! This angers me to no end! Why can they hear from ME, from US, from OUR Doctor’s??? I have written comments to every single FDA hearing that allows public comments, but I do not even know if my voice is been heard! I am so frustrated!
Most excellent Dr. Fudin, I think there was points that needed to be made and you covered them really good. After all that was said during this hearing the last two days I do believe the FDA did not get enough solid evidence they need to make such drastic changes.
In time I do believe we will get a handle on this situation and things will smooth over. We cant leave suffering people to suffer even more , people need pain relief when they have tried everything and nothing has worked till they try a aggressive opioid therapy. Chronic pain is something that needs to be cared for with compassion and understanding.
Thanks for all that you have done to give people a better understanding of opioid therapy.
Mark S. Barletta
Thank you for being there to represent an educated, rational perspective on this issue, Dr. Fudin.
Jeff, you rock.
Again, speaking truth to power-and in the case of PROP-to those wishing they could influence it has raised the spirits of at least this one PROMPT member.
Perhaps you could share additional observations of from the hearing
Gratefully
Mike Brennan
The retired Navy vet, that had PTSD problems, or “Psychotic Depression”, which it sounds to me would be the correct diagnosis. YOU HIT THE NAIL ON THE HEAD. THE presentation of this prop docs are terribly misleading.
I have PTSD. I was diagnosed with it from South East Asia, and from the injury in “99”, which caused this mess in my back. The Dr. that Workerscomp sent me too was very vocal in his diagnosis of PTSD from the injury, and the injury bringing back the former, and first diagnosis. BUT, i am not suicidal, homocidal , nor do I hallucinate. They just don’t hear all the stories of Arachnoiditis patients that have non cancer irretractable pain. I now I am not a good speller, for a “3.7 GPA” Nursing student so long ago, but damn it, they even correct my spelling on “Arachnoiditis”. Which is correct. So, that show’s you how many people, who count, that really know what this disease really is. We thankyou for your help Dr. Jeff, and I pray the FDA doesn’t do something foolish…..thanks again, doc,,,,,,,,herb neeland